My son says he hasn't had to wear his mask in over a week and a half. Most teachers aren't saying anything anymore.")
Hence the Covid problems with your school system in Florida will continue --- and you will soon be going remote.
My son says he hasn't had to wear his mask in over a week and a half. Most teachers aren't saying anything anymore.
So let's read the Conclusions on the first page of the study:
Conclusions: Our intervention demonstrates a scalable and effective method to promote mask
adoption and reduce symptomatic SARS-CoV-2 infections.
(Nothing more needs to be said)
Hence the Covid problems with your school system in Florida will continue --- and you will soon be going remote.
Science regarding masks. Not sCiEnCe. Be warned, requires critical thinking skills, so you might not understand if all you are about is a narrative:

Emily Burns #SmilesMatter DM’s OK
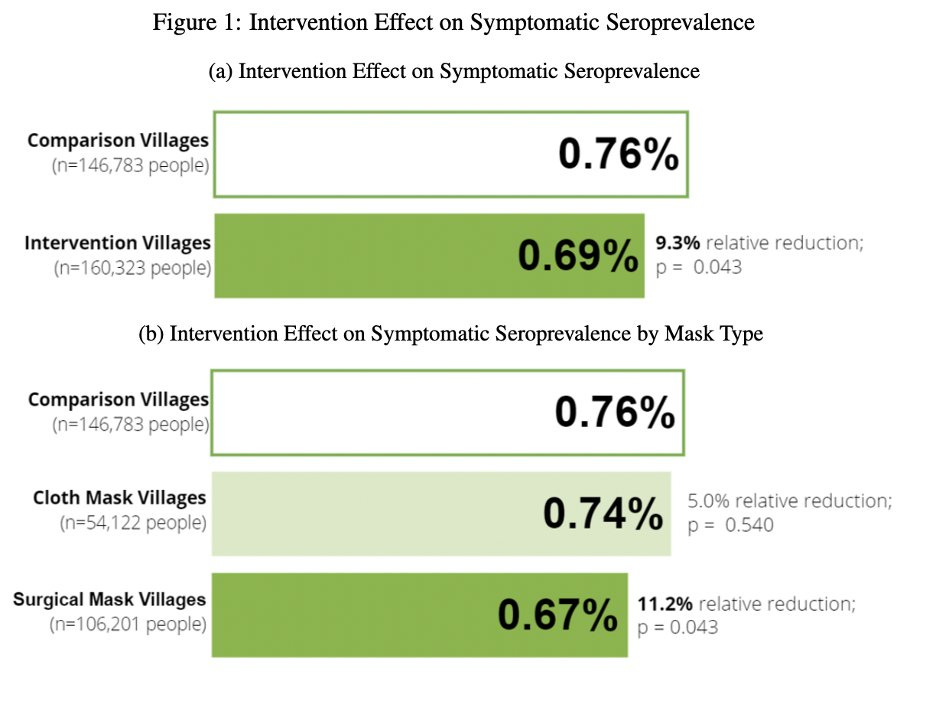
The overall effects of this study are miniscule—0.07% absolute reduction in seroprevalence. But the topline finding is “We decreased seroprevalence by 10%!”
Technically true...
But even this finding is questionable. Let's explore.
poverty-action.org/sites/default/…
What the study ACTUALLY measures is the impact of mask promotion on symptom reporting. Only if a person reports symptoms, are they asked to participate in a serology study—and only 40% of those with symptoms chose to have their blood taken.
Is it possible that that highly moralistic framing and monetary incentives given to village elders for compliance might dissuade a person from reporting symptoms representing individual and collective moral failure—one that could cost the village money? Maybe?
Given that the difference is tiny, if this had even a small impact, it could completely skew the results. Might the same factors be at play when an individual weighed whether or not to be tested? After all, a positive test would indicate that your village was “failing”
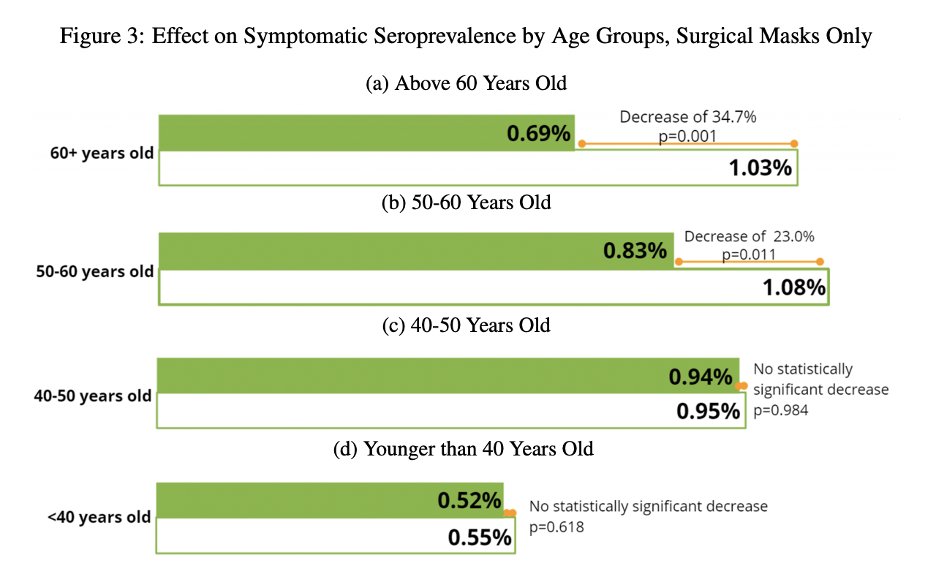
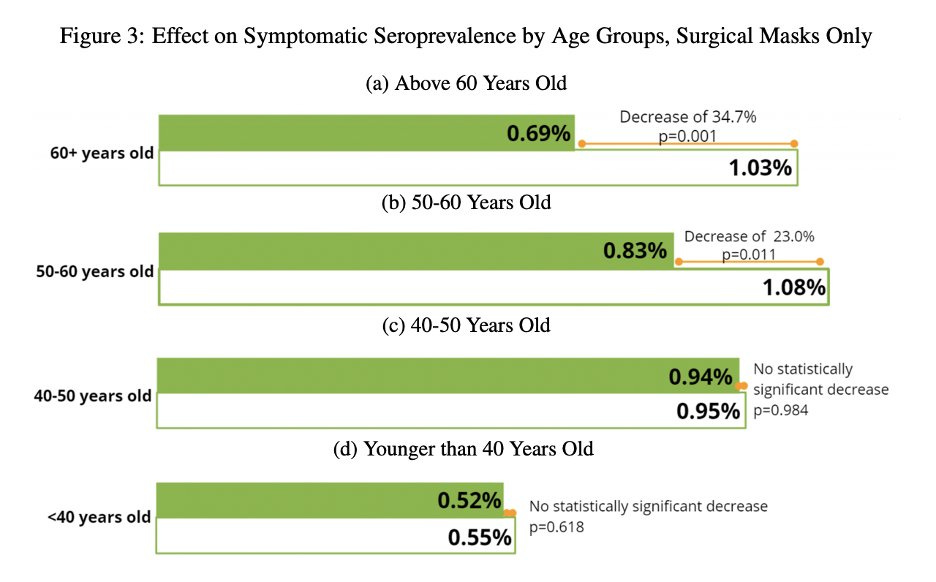
The fact that age stratification shows that interventions had no impact on younger people, but did on older people calls this finding into question. There is no physical mechanism by which universal masking would protect the elderly, but not the young.
Such a result could be explained by the mask promotion campaign creating a sense of fear that resulted in elderly sequestering themselves. If that were the case, a more elderly-targeted approach could achieve the same results.
It is also possible that elderly people in intervention groups were less likely to report symptoms. 60+ are 2-3x more likely to be symptomatic than <40. Again, when having symptoms means you failed your village, might you choose not to mention them?
Age and Likelihood of Developing Symptoms and Critical Disease After SARS-CoV-2 Infection in ItalyThis cohort study examines the association of age with the likelihood of experiencing symptoms and progressing to critical illness after infection with severe acute respiratory syndrome coronavirus 2 …https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2777314
Perhaps the most compelling aspect of the study is the difference between surgical and cloth mask villages. The authors claim that this is supported by the different filtration efficiencies of cloth and surgical masks.
However, these filtration efficiencies are taken in a no-gap scenario. And there is ALWAYS a gap. We can see that when considering gaps—the most important element of filtration--fabric & surgical masks perform nearly identically--not at all.
Given physical improbability, it is possible that this effect too, might be an artifact of bias in the control group. Surgical masks are “fancier," & might feel like more of an intervention, and may make those in such a village even more likely to repress symptom reporting.
Whatever the result of the surgical masks, this shows that the impact from cloth masks is 0. (.02% absolute reduction and a p-value of 0.540 is zero, even if the authors want to pretend otherwise).
Color me skeptical on this one. This study increased mask wearing to 40%. In much of blue America mask compliance approached 100% for almost a year. Even with that kind of incredible compliance, there was no impact on case transmission rates.
Let's see what the scientific community is saying about this study of masks in Bangladesh. Yes, science is important. This large scale study proves conclusively that masks are effective in stopping the spread of Covid.
The study that 'should basically end any scientific debate' about masks
https://theweek.com/coronavirus/100...sically-end-any-scientific-debate-about-masks
A massive randomized trial on how well masks hold up against symptomatic COVID-19 infections may be one of the most crucial studies of the coronavirus pandemic because it was able to solve the tricky issue of examining mask-wearing at a community level rather than an individual one.
The study involved launching pro-mask campaigns in some Bangladeshi villages, but not others, and the authors made two key findings. First, they determined that the public health interventions nearly tripled mask usage from 13 percent to 42 percent. Secondly, they discovered — by conducting sero-surveys backed up by interviews about COVID-19 symptoms and medical history — that masks did their job and reduced symptomatic infections in the communities that were subject to the campaigns by 9.3 percent. Jason Abaluck, an economist at Yale University who helped lead the study, toldThe Washington Post that figure would probably be higher if masking was universal.
There were a few other key notes in the study. Surgical masks were found to be particularly effective, while the jury is still out on cloth masks. And they were more effective in people older than 50, which could be explained by a few factors, including that young people were less likely to be symptomatic either way. They also may have been less compliant when it comes to masks.
Either way, Abaluck is pretty confident about the research, arguing that it "should basically end any scientific debate about whether masks can be effective in combating [COVID-19] at the population level" and calling it "a nail in the coffin" for anti-mask arguments. Read more atThe Washington Post.


 Emily Burns #SmilesMatter DM’s OK @Emily_Burns_V
Emily Burns #SmilesMatter DM’s OK @Emily_Burns_V Emily Burns #SmilesMatter DM’s OK @Emily_Burns_V
Emily Burns #SmilesMatter DM’s OK @Emily_Burns_V



This is a very easy read that shows you why the study is such a joke. That is, if you understand how to do a medical RCT (which clearly, you do not).
Let’s start with the basics on how to do a medical RCT.
Establish the Starting Condition/Randomize Cohorts into even groups:
- establish the starting condition. if you do not know this, you have no idea what any later numbers or changes mean. it also makes step 2 impossible.
- randomize cohorts into even groups in terms of start state and risk. this way, they are truly comparable. randomizing by picking names out of a hat is not good enough. you can wind up doing a trial on a heart med where 20% of active arm and 40% of control have hypertension. you cannot retrospectively risk adjust in a prospective trial. this needs to be done with enrollment and study arm balancing. fail this, and you can never recover.
- isolate the variable you seek to measure. to know if X affects Y, you need to hold all other variables constant. only univariate analysis is relevant to a unitary intervention. if you give each patient 4 drugs, you cannot tell how much effect only drug 1 had. you’ve created a multivariate system. get this wrong, and you have no idea what you measured.
- collect outcomes data in a defined, measurable, and equal fashion. uniformity is paramount. if you measure unevenly and haphazardly, you have no idea what manner of cross confounds and bias you have added. you will never be able to separate signal from measurement artifacts. this means your data is junk and cannot support conclusions.
- set clear outcomes and measures of success. you need to decide these ahead of time and lay them out. data mining for them afterwards is called “p-hacking” and it’s literal cheating. patterns emerge in any random data set. finding them proves nothing. this is how you perform a study that will not replicate. it’s a junk analysis.
and balance cohorts: this was a total fail and doomed them before they even began.
this is their key claim in the finding. but notice what is jarringly absent: any clear idea what prior disease exposure was in each of these villages and village cohorts at study commencement. small current seroprevalence probes cannot tell us this. there is no way to know if one had had a big wave and another had not. so, we literally have no idea what had happened here and on what sort of population. we have no idea if we are studying a naïve population or not.
performing this study without a clear and broad based baseline and sense of past exposure is absurd. this is a tiny signal (7 in 10,000) we need a very high precision in start state. it’s absent. that’s the ballgame right there. we do not know and can never know what happened. even miniscule variance in prior exposure would swamp this.
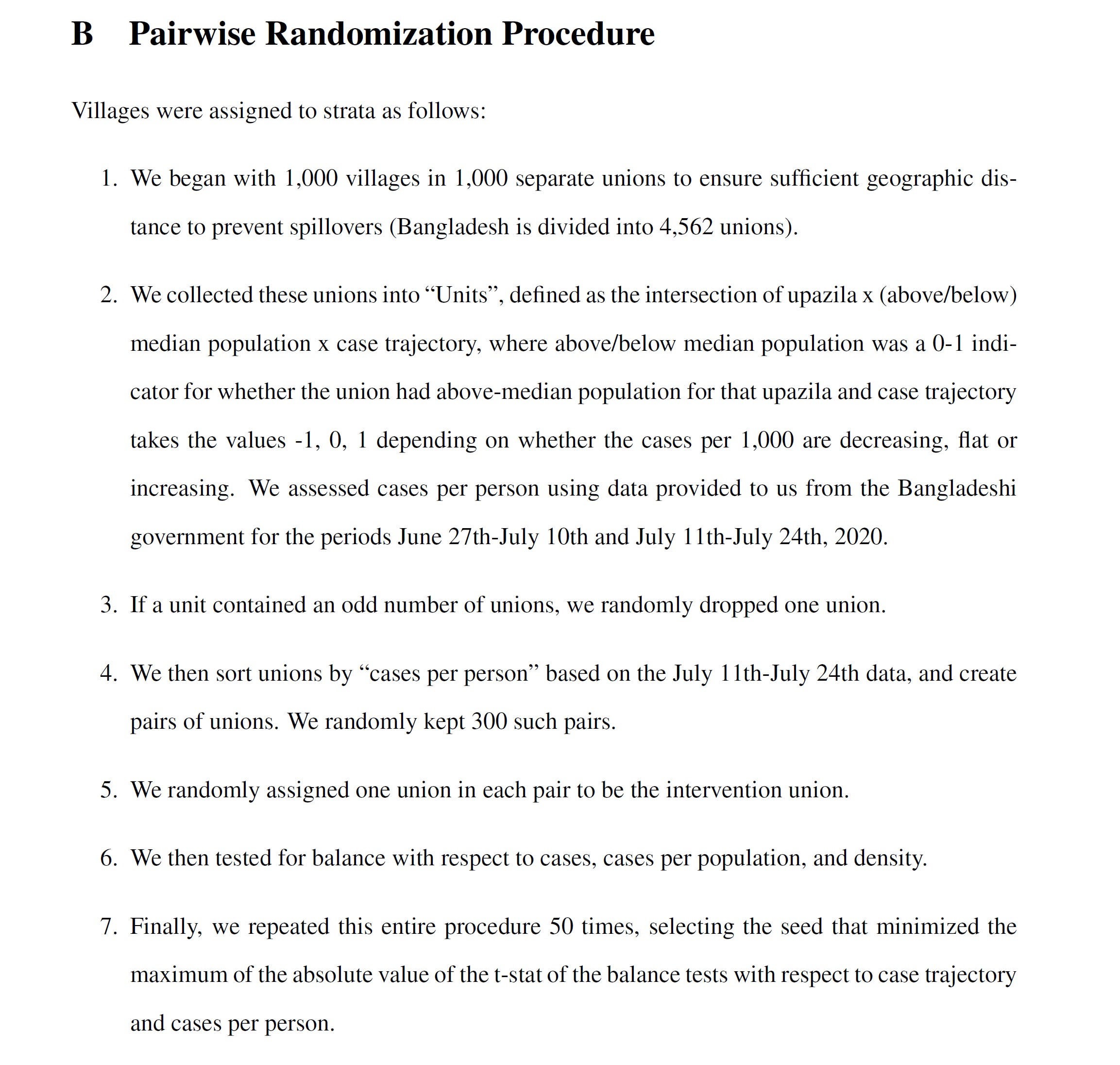
for cohorts, they paired by past covid cases (so thinly reported as to be near meaningless and a possible injection of bias as testing rates may vary by village) and tried to establish a “cases per person” pair metric to sort cohorts. this modality is invalid on its face without reference to testing levels. you have no idea if high cases are high testing or high disease prevalence. you have no idea how much testing varied.
and testing levels are so low, the authors estimate a 0.55% case detection rate. so a modality invalid even if data were good is multiplied in terms of error because the data is terrible (and likely wildly variable by geography)
nowhere here does the word “testing” or “sample rate” appear.
so this study ended before it even began.
this was not useful randomization. this was garbage in garbage out especially when you later seek to use “symptomatic seroprevalence” as primary outcome. that’s false equivalence. if you’re going to use seroprevalence as an outcome, you need to measure it as a start state and balance the cohorts using it. period. failure to do so invalidates everything. you cannot run a “balance test” on current IgG and presume you know what happened last year, certainly not to the kind of precision needed to find a 0.0007 signal meaningful.
this was an unknown start state in terms of highly relevant variables and the cohorts were not normalized (or even measured) for it.
they also failed to measure masked vs unmasked seroprev in any given village. that would have been useful control data. it seems like they really just missed all the relevant info here.
it’s pure statistical legerdemain.
strike 1 and 2.
but it gets worse. much worse.
isolate the variable you seek to measure.
to claim that masks caused any given variance in outcome, you need to isolate masks as a variable. they didn’t. this was a whole panoply of interventions, signage, hectoring, nudges, payments, and psychological games. it had hundreds of known effects and who knows how many unknown ones.
we have zero idea what’s being measured and even some of those variables that were measured showed high correlation and thus pose confounds. when you’re upending village life, claiming one aspect made the difference becomes statistically impossible. the system becomes hopelessly multivariate and cross-confounded.
the authors admit it themselves (and oddly do not seem to grasp that this invalidates their own mask claims)
who knows what the effects of the “intervention package” were outside of masking? maybe it also leads to more hand washing or taking of vitamins. it seemed to effect distancing (though i doubt that mattered).
but the biggest hole here is that that which affects one attitude can affect another.
if you’ve been co-opted to “lead by example” and put up signage etc or are being paid to mask you may change your attitude about reporting symptoms.
people want to please researchers and paymasters and this is a classic violation of a double blind system. the subjects should no know if they are control or active arm, but in the presence of widespread positive mask messaging, they do.
so maybe they think “i don’t not want to tell them i’m sick.” especially if “being sick” has been vilified.
or maybe they fail to focus on minor symptoms because they are masked and feel safe or were having more trouble breathing anyhow.
this makes a complete mess and injects all manner of unpredictable bias into the “results” because the results are based on “self reporting” a notoriously inaccurate modality.
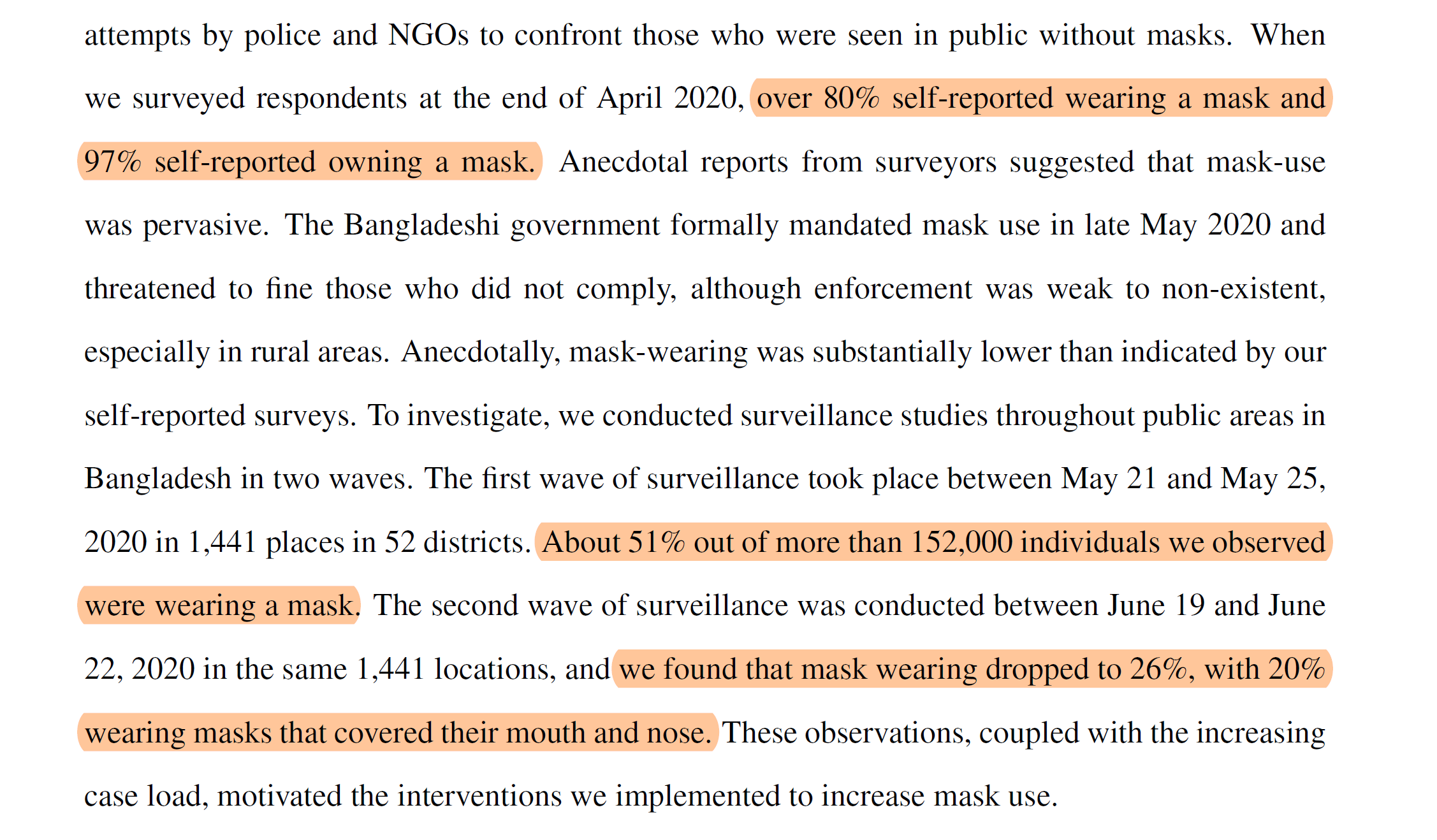
look at the wide variance in self reporting on masks and reality cited in this very study.
yet we’re to accept self reporting of symptoms in the face of widespread and persistent moral suasion in one arm and not the other and assume that the same interventions that had a large effect on mask wear affected no other attitudes?
no way. this non-blinded issue combining with self reporting adds one tailed error bars so large to this system that they swamp any signal.
as is so often the case, gatopal @Emily_Burns-V has a great take here:
2/2/ What the study ACTUALLY measures is the impact of mask promotion on symptom reporting. Only if a person reports symptoms, are they asked to participate in a serology study—and only 40% of those with symptoms chose to have their blood taken.
September 1st 2021
11 Retweets58 Likes
3/ Is it possible that that highly moralistic framing and monetary incentives given to village elders for compliance might dissuade a person from reporting symptoms representing individual and collective moral failure—one that could cost the village money? Maybe?
September 1st 2021
8 Retweets44 Likes
this is exactly why good studies are blinded. if they are not, the subjects seek to please the researchers and it wrecks the data. adding self reporting is a multiplier on this problem. this whole methodology is junk and so is the data it produced.
for proof of this, one need only look at the age stratification:
first off, this proves conclusively that “your mask does not protect me.” (though we already knew that) if it did, it would protect everyone, not just old people. but it didn’t. and the idea that it stopped old people from getting sick but not young people is similarly implausible.
the odds on bet here is that old people were more inclined to please the researchers than young people and that they failed to report symptoms as a result.
i establish this as the null hypothesis.
can anyone demonstrate that this data makes a more compelling case for “masks worked on old people but not young people and thus decreased overall disease”?
because i very much doubt it.
and unless you can, you must abandon this study as a possibly interesting piece of sociology, but as having zero validated epidemiological relevance.
so, that’s strikes 3 and 4.
i’m honestly a bit unsure about whether we can go on to call it a perfect 5. they did pre-register the study and describe end states, but they never established start states so we have no idea what actual change was.
so, they called their end results shot beforehand (as they should) but then left us with no way to measure change even if the measurement was good, and as we have seen, the measurement was terrible.
so i’m going to sort of punt on scoring this one and assign it an N/A. establishing an outcome and then providing no meaningful way to measure it is not p-hacking per se, but it is also not in any way useful.
so, all in all, it’s just impossible to take this study seriously, especially as it flies in the face of about 100 other studies that WERE well designed.
read many HERE including RCT’s showing not only a failure as source control, but in higher rates of post op infections from surgeons wearing masks in operating theaters vs those that did not.
the WHO said so in 2019.
and the DANMASK study in denmark was a gold standard study for variable isolation and showed no efficacy.
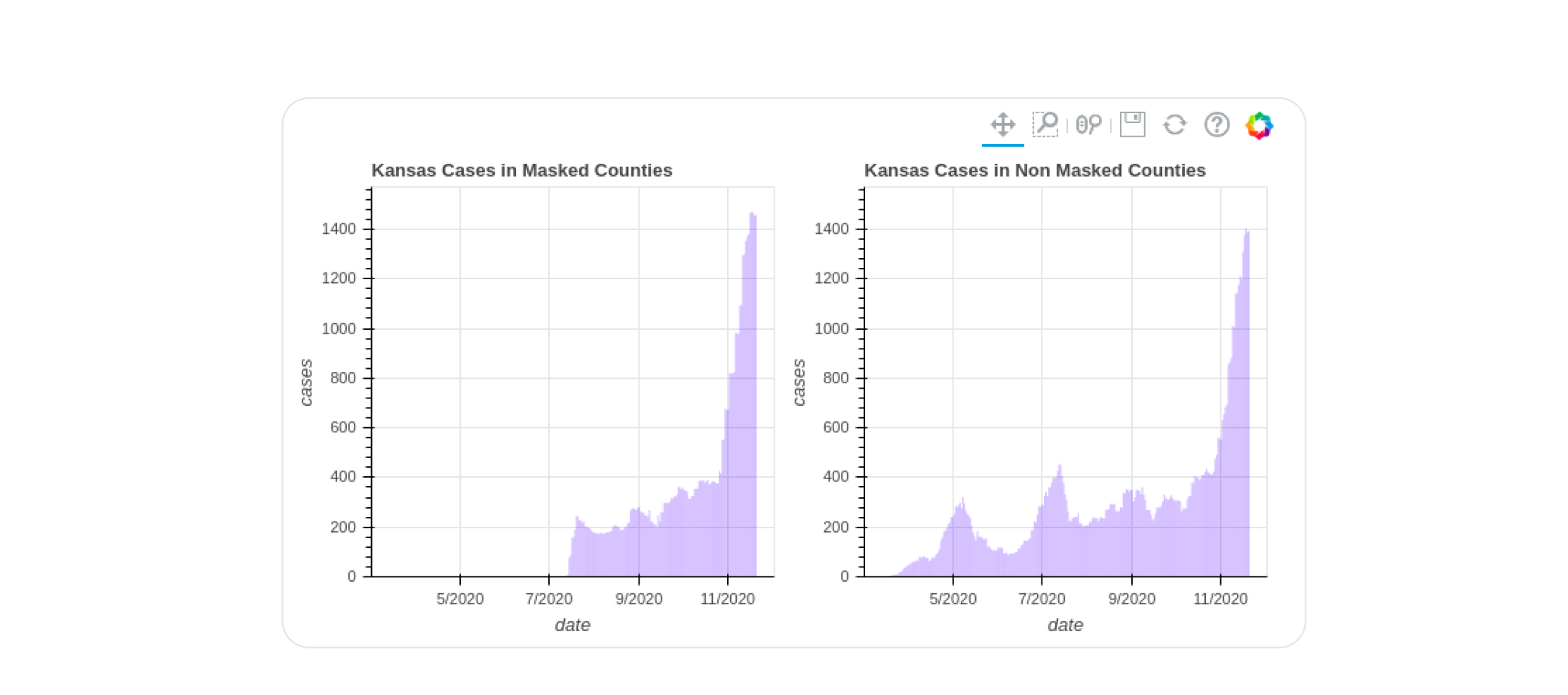
perhaps most hilariously, the very kansas counties data the CDC tried to cherry pick to claim masks worked went on to utterly refute them when the covid surge came.
the evidence that masks fail to stop covid spread is strong, deep, wide, and has a lot of high quality studies. (many more here from the swiss)
to refute them would take very high quality data from well performed studies and counter to the current breathless histrionics of masqueraders desperate for a study to wave around to confirm their priors, this is not that.
to claim “masks worked” with ~40% compliance in the light of total fails with 80-95% is so implausible as to require profound and solid evidence that is nowhere provided here.
this is a junk output from a junk methodology imposed upon an invalid randomization without reference to a meaningful start state for data.
this is closer to apples to orangutans than even apples and oranges.
thus, this and many more like is an absurd and impossible take from this study.
it does not show efficacy. it does not show ANYTHING outside of how an object lesson in poor study design and data collection can be weaponized into a political talking point.
this study is an outright embarrassment and a huge black eye for the NBER et al.
this is not even wrong.
it’s just an epic concatenation of bad techniques and worse data handling used to provide pretext for an idea the researchers clearly favored. there is no way to separate bias from fact or data from artifact.
calling this proof of anything is simply proof of either incompetence or malfeasance.
which one makes you want to listen to the folks pushing it?
I will stick with what the scientists are stating. Rather than the misinformation (actually it is classic FUD stuff) above which you copied/pasted from anti-mask COVID-deniers.
Right. As usual, you are unable to pick out a single item to dispute.
We're on to your game, fraud-ling.