You are pushing the planning scenarios nonsense again simply looking at one of the five planning scenarios proposed. Your numbers are complete junk -- they are not the actual numbers --- merely numbers from a planning scenario.
Let's take a look at the actual estimated U.S. Infection Fatality Rate numbers in the U.S.
The CDC has estimated that the nationwide IFR for the United States is 0.65 percent.
The CDC's Latest Antibody Data Confirm Huge Interstate Differences in COVID-19 Fatality Rates
The findings suggest that people infected in Connecticut were 10 times as likely to die as people infected in Utah or Oregon.
https://reason.com/2020/10/20/the-c...state-differences-in-covid-19-fatality-rates/
The latest data from antibody studies conducted by the Centers for Disease Control and Prevention (CDC) across the country confirm that the death rate among Americans infected by the COVID-19 virus
varies very widely from one state to another. The CDC's
prevalence estimates for August, combined with contemporaneous death counts, suggest that the infection fatality rate (IFR) was at least 10 times higher in Connecticut than in Idaho, Nebraska, Oregon, Tennessee, or Utah, for example.
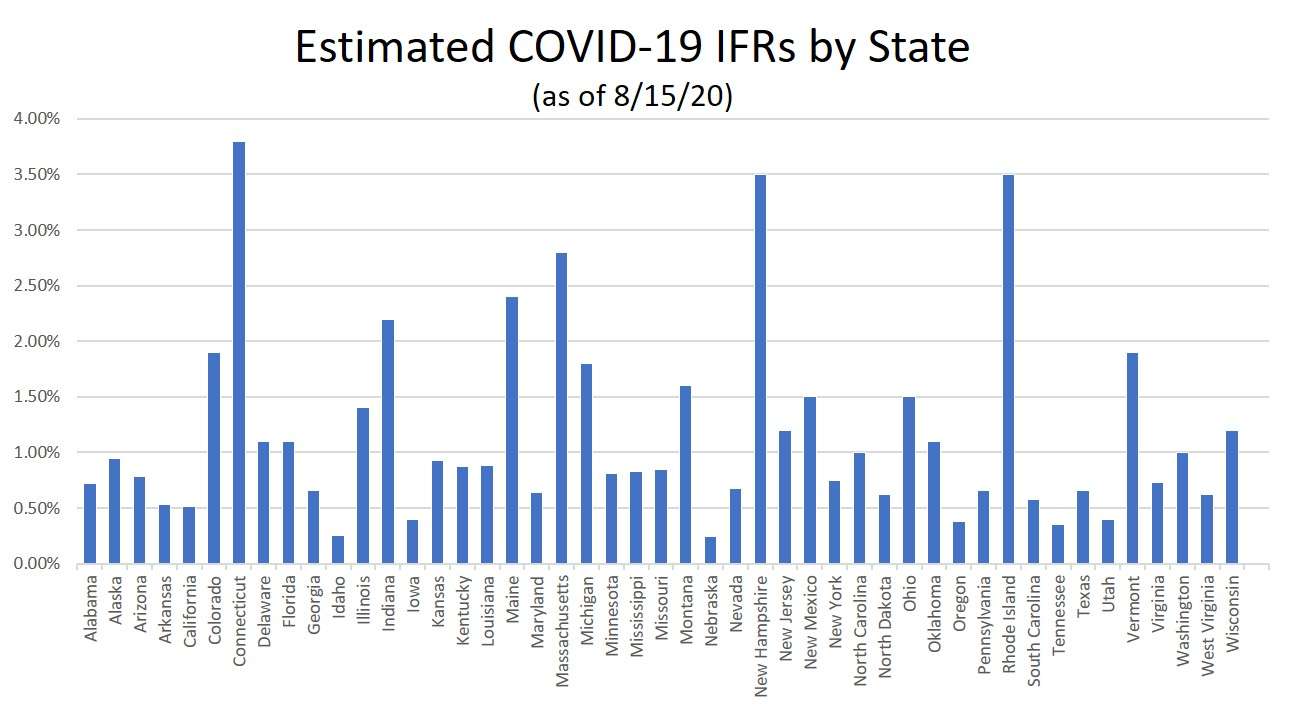
The CDC estimated the number of people who had been infected in each state based on antibody screening of blood samples drawn for routine diagnostic tests unrelated to COVID-19. Those patients may not have been representative of the general population, and the number of samples tested was relatively small in most states, leading to wide confidence intervals. Still, the CDC's numbers give us a sense of the gap between confirmed cases and total infections (including cases with mild or no symptoms) in each state. I combined those estimates with the death tolls reported by
Worldometer as of August 15 to estimate IFRs.
The estimated IFRs range from less than 0.4 percent in Idaho, Nebraska, Oregon, Tennessee, and Utah to 3.8 percent in Connecticut. Most states (27) had estimated IFRs below 1 percent, although 20 reached or exceeded that threshold. The CDC did not report prevalence estimates for Hawaii, South Dakota, or Wyoming.
Based on data from other countries,
the CDC has estimated that the nationwide IFR for the United States is 0.65 percent, although the estimate
varies dramatically with age, from 0.003 percent among people 19 or younger to 5.4 percent among people in their 70s. If you look at the 10 states with the biggest populations, you can see that the estimated IFR based on the CDC's prevalence numbers is similar to the CDC's nationwide IFR estimate in Texas, Pennsylvania, and Georgia; lower in California; and higher in New York, Florida, Illinois, Ohio, North Carolina, and Michigan.
The estimated IFR for New York, the state with the highest infection rate, is 0.75 percent. That IFR is somewhat higher than the estimate suggested by an
antibody study that the New York State Department of Health conducted in April, when it put statewide infection prevalence at 14 percent, compared to the CDC's estimate of 22.5 percent in August.
Given the uncertainties of extrapolating from the blood samples analyzed by the CDC, which were not randomly drawn from the general population, we should not put too much stock in these state-specific IFR estimates. But the high estimated IFRs for Northeastern states such as Connecticut, Massachusetts, New Hampshire, and Rhode Island are consistent with their
high case fatality rates (deaths as a share of confirmed cases). Conversely, the lower IFR estimates for states such as Arkansas, California, Idaho, Kansas, Nebraska, Oregon, Tennessee, and Utah are consistent with their lower case fatality rates.
Why do COVID-19 patients fare so much worse in some states than others? Possible explanations include age demographics, the prevalence of preexisting medical conditions, the quality and capacity of local health care systems (including the extent to which they are strained by the pandemic), and population density, which not only makes it easier for the virus to move from person to person but may result in
larger virus doses and more dangerous infections. Another factor could be the timing of each state's epidemic, since the development of more effective treatments may have improved outcomes for people infected more recently.